 I-Gear & AIDS:
I-Gear & AIDS:
Access to HIV /AIDS Educational
Websites in New York City Public Schools
A
WebQuest for 6th Grade (Communication Arts)
Designed
by
Jonathan
C Schleifer
mrschleifer@teacher.com
-Introduction:
 You are public school teacher in
You are public school teacher in New York City V /AIDS prevention. You will review research that describes the
importance of access to information in HIV /AIDS prevention, review the New
York City Policy towards filtering Internet content, and test this policy by
trying to find websites that you can use to teach your students HIV /AIDS prevention. Once you have completed your research you
will draft an email to the New York City
-Task: 
Once
you have completed your research you will draft an email to the New York City
Board of Education requesting that they change their filtering policy you will
include in it the reasons including HIV /AIDS educational resources as so
important and the list of sites that are blocked that need to be accessible.
-Process
& Resources: (please check
each box R as you complete it.)
Step 1:
q
With your
partner you will print worksheets 1 and 2. They will help you clearly define of the problem
(worksheet 1) and collect
evidence (worksheet 2)
q
Read the following World Wide Web pages
and answer the questions on worksheet #1. Only parts of the page will help you
answer this question so read carefully. Please pay attention to the parts that
focus on increased risks in adolescents. Because
these sites may be blocked in your school I have quoted them at the bottom of
this WebQuest in Appendixes I, II, and III.
Ä What
Are Adolescents' HIV Prevention Needs? (Appendix I)
Ä Early Sexual
Initiation and Subsequent Sex-Related Risks Among Urban Minority Youth: The
Reach for Health Study (Appendix II)
Ä New Study Examines Adolescents’ Use of the Internet for
Health Information (Appendix
III)
Step 3:
q
With your partner
you will print the following worksheet and read it will help you to evaluate current
public policies - Worksheet 4.
q
Read the
following World Wide Web pages and answer the questions on worksheet 4.
Ä The NYC Board of Education
Internet Acceptable Use Policy section on filtering
q
Use a common
search engine such as:
![]()
![]() Search for web sites that might provide information
for your students on HI
Search for web sites that might provide information
for your students on HI
Step 4:
q
With your
partner you will print the following worksheet and read it will help you to develop your own
public policies – Worksheet
5
q
Complete Worksheet 5
with your partner.
Step 5:
q
With your
partner you will print the following worksheet and it will help you to choose the best
solution – Worksheet
6.
q
Evaluate your
different policy recommendations and complete Worksheet 6.
Step 6:
Now that you have chosen the best solution you must
take action.
Write an email to the
Board of Education and propose your policy.
Explain clearly the faults in the current policy emphasizing your test
of the filtering software. Explain the dangers
of filtering this information from you students and advocate for you policy.
Ä
Members
of the Board of Education City of New York
-Evaluation:
|
|
Excellent 4 |
Good 3 (needs more work) |
Satisfactory 2(needs
a lot more work) |
Unacceptable 1 (needs to be redone) |
|
Define the problem |
Scholar stated the problem clearly and with some detail. |
Scholar stated the problem but without
detail. |
|
Scholar did not state the problem. |
|
Scholar identified the correct specific community location. |
Scholar did not identify the correct specific community location. |
|
Scholar did not identify any specific community location. |
|
|
Scholar identified three
undesirable social conditions that result from this problem |
Scholar identified two
undesirable social conditions that result from this problem |
Scholar identified one
undesirable social conditions that result from this problem |
Scholar did not
identify any undesirable
social conditions that result from this problem |
|
|
Gathering evidence of the problem |
Scholar presents three pieces of evidence that a problem exists. |
Scholar presents two
pieces of evidence
that a problem exists. |
Scholar presents one
pieces of evidence
that a problem exists. |
Scholar does not present any evidence that a problem exists. |
|
Evaluating
existing public policies |
Scholar has stated one of the major existing policies that attempts to deal with the social problem. |
|
|
Scholar has not
stated one of the major existing policies that attempts to deal with the
social problem. |
|
Scholar identified two or more advantages of this policy. |
Scholar identified one
of the advantages of this policy. |
|
Scholar identified two
or more advantages of this policy |
|
|
Scholar identified two
or more disadvantages of this policy. |
Scholar identified one
of the disadvantages of this policy. |
|
Scholar identified two
or more disadvantages of this policy. |
|
|
Scholar has stated whether the policy should be replaced, strengthened, or improved and supported their answer. |
Scholar has
stated whether the policy should be replaced, strengthened, or improved
but did not support their answer. |
|
Scholar has not
stated whether the policy should be replaced, strengthened, or improved. |
|
|
Developing public policy solutions |
Scholar has proposed at least three new/original public policy alternatives. (Scholar must elaborate on their new/original policies) |
Scholar has proposed two new/original public policy alternatives. (Scholar must elaborate on their new/original policies) |
Scholar has proposed one new/original public policy alternatives. (Scholar must elaborate on their new/original policy) |
Scholar has not proposed new/original public policy
alternatives. |
|
Selecting the best public policy solution |
Scholar has chosen between
the alternative policies they created and defended their choice. |
Scholar has chosen
between the alternative policies they created but did not defend their
choice. |
|
Scholar has not
chosen between the alternative policies they created. |

-Conclusion:
In
this WebQuest you have studied the policies of the New York City
-Image
Sources: Give ©redit
where ¢redit is due.
1.
www.urmc.rochester.edu/
strong/AIDS/aidspg.htm
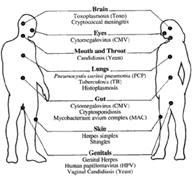
2.
http://www.aegis.com/topics/oi/
3.
www.cdc.gov/od/admh/
health.htm
4.
pravda.ru/main/2001/
08/24/31067.html
-New York State
E1c
Read and comprehend informational materials.
E1d Demonstrate familiarity with a
variety of public documents.
E1e Demonstrate familiarity with a variety of
functional documents.
E2a
Produce a report of information.
E2e Produce a persuasive essay.
E3b
Participate in group meetings
E3b
Participate in group meetings
E4b
Analyze and subsequently revise work to improve its clarity and effectiveness.
-Appendix
I
The
following is found at
http://www.caps.ucsf.edu/adolrev.html
 What
Are Adolescents' HI
What
Are Adolescents' HIV Prevention Needs?
(updated 4/99)
Can adolescents get HIV ?
Unfortunately, yes. HI
Unprotected sexual intercourse puts young people at risk not only for HI
Some sexually-active young African-American and
What puts adolescents at risk?
Adolescence is a developmental period marked by discovery and experimentation that comes with a myriad of physical and emotional changes. Sexual behavior and/or drug use are often a part of this exploration. During this time of growth and change, young people get mixed messages. Teens are urged to remain abstinent while surrounded by images on television, movies and magazines of glamorous people having sex, smoking and drinking. Double standards exist for girls-who are expected to remain virgins-and boys-who are pressured to prove their manhood through sexual activity and aggressiveness. And in the name of culture, religion or morality, young people are often denied access to information about their bodies and health risks that can help keep them safe. 5
A recent national survey of teens in school showed that from 1991 to 1997, the prevalence of sexually activity decreased 15% for male students, 13% for White students and 11% for African-American students. However, sexual experience among female students and Latino students did not decrease. Condom use increased 23% among sexually active students. However, only about half of sexually active students (57%) used condoms during their last sexual intercourse. 6
Not all adolescents are equally at risk for HI
Can education help?
Yes. Schools are an important venue for educating teenagers
on many kinds of health risks, including HI
Are schools the only answer?
No. Young people need to get prevention messages in lots of
different ways and in lots of different settings. Schools alone can't do the
job. In the
Youth who are not in school have higher frequencies of behaviors that put
them at risk for HI
Programs targeting hard-to-reach adolescents at high risk for HI
Families play an important role in helping teenagers avoid risk behaviors.
Frank discussions between parents and adolescent children about condoms can
lead teens to adopt behaviors that will prevent them from getting HI
The WEHO Lounge in
Project
What needs to be done?
HI
Any program for adolescents should be interesting, fun and interactive, and
involve youth in the planning and implementation. This is especially true for
out-of-the-mainstream youth and youth from diverse cultures. Programs for hard-to-reach
youth who are most at risk for HI
Says who?
1. Centers for Disease Control and Prevention. Young people at
risk-epidemic shifts further toward young women and minorities. Fact sheet prepared by the CDC. July 1998.
2. Eng TR,
3.
4. Miller KS, Clark LF, Moore JS. Sexual
initiation with older male partners and subsequent HI
5. UNAIDS. Force for Change: World AIDS Campaign with Young
People. Report prepared by UNAIDS, The Joint United Nations Programme
on HI
6. Centers for Disease Control and Prevention. Trends
in sexual risk behaviors among high school students-United States, 1991-1997.
Morbidity and Mortality Weekly Report. 1998;47:749-752.
7. Rotheram-Borus MJ, Mahler KA,
Rosario M. AIDS prevention with adolescents. AIDS
Education and Prevention. 1995;7:320-336.
8. UNAIDS. Impact of HI
9. Pinkerton SD, Cecil H, Holtgrave
D.R. HI
10. Associated Press. Sex education that teaches abstinence wins
support. New York Times.
11. Jemmott JB, Jemmott
LS, Fong GT. Abstinence and safer sex HI
12. Centers for Disease Control and Prevention. Health risk behaviors among adolescents who do and do not attend
school-United States, 1992. Morbidity and Mortality
Weekly Report. 1994;43:129-132.
13. Zibalese-Crawford M. A creative
approach to HI
14. Miller KS, Levin ML, Whitaker DJ, et al. Patterns of condom
use among adolescents: the impact of mother-adolescent communication. American Journal of Public Health. 1998;88:1542-1544.
15. Weinstein M, Farthing C, Portillo T, et al. Taking it to the
streets: HI
16. Harper GW, Contreras R,
Prepared by Gary
W. Harper, PhD MPH* and Pamela DeCarlo**
*Department of Psychology,
April 1999. Fact Sheet #9ER
Reproduction of this text is encouraged;
however, copies may not be sold, and the Center for AIDS Prevention Studies at
the
![]() Return
to Fact Sheets main page
Return
to Fact Sheets main page
-----------------------------------------------
-Appendix
II
The
following is found at http://www.thebody.com/siecus/middle_school_behavior.html
|
|
||
|
|
SHOP
Talk: School Health Opportunities and Progress Bulletin |
|
Early Sexual Initiation and Subsequent Sex-Related Risks Among Urban Minority Youth: The Reach for Health StudyFamily Planning Perspectives recently published results from the Reach for Health (RFH) Study that examines early sexual initiation and its possible relationships to risky sexual behaviors among urban minority youth. The study included 1,287 minority seventh graders who attended one of
three participating middle schools in ResultsEver Had IntercourseMales
Females
Had "Recent" IntercourseMales
Females
Males
Females
Used a Condom Less Than Half of the TimeMales
Females
Involved in PregnancyMales
Females
Males
Females
10th Grade Population OnlyHad 4 or More Sex Partners
Was Drunk/High During Sex
The authors note that although youth who initiate intercourse early may have more experience, they do not use condoms more consistently. These same youth also experience a disproportionate number of pregnancies. They point out that the health and social consequences of early sexual onset are not equally distributed nationally among youth. According to the authors, the chance that a white adolescent experiences his or her first intercourse at the ages commonly reported in this sample is small. Therefore, they believe, it is clear that early sexual initiation and its subsequent pattern of risk-taking have not been receiving the attention they deserve or would get if the behaviors were more prevalent in wealthier communities. The authors believe the assumption that early adolescents are not sexually active has resulted in serious limitations on what prevention and intervention programs can address at different developmental stages. They think a fuller understanding of various cultures, including gender roles and their link to early sexual experimentation, are essential for the development of programs that address the needs of both males and females from minority communities. For more information: L. O’Donnell, et al., “Early Sexual Initiation and Subsequent Sex-Related Risks Among Urban Minority Youth: The Reach for Health Study,” Family Planning Perspectives, vol. 33, no. 6, pp. 268-75. |
||

This document was provided by The Sexuality Information
and Education Council.







-----------------------------------------------
-Appendix III
The
following is found at http://www.thebody.com/siecus/internet.html
|
|
SHOP
Talk: School Health Opportunities and Progress Bulletin |
|
New Study Examines Adolescents’ Use of the Internet for Health InformationA study in the July issue of the Archives of Pediatric and Adolescent Medicine examines adolescents' use of and attitudes toward accessing health information through the Internet. Researchers surveyed 412 tenth grade students in an economically and ethnically diverse suburban town. The survey focused on three health areas: birth control and safer sex; diet, nutrition, and exercise; and dating and family violence. Students were asked what health topics they had ever tried to obtain information on from the Internet, what topics they obtained "the most information on from the Internet," and whether they thought the Internet was worthwhile, trustworthy, useful, and relevant. Internet Use
Where Teens Get InformationRespondents were asked which of 15 possible sources they used for health information. They could name more than one source. Among responses:
|
||
This document was provided by The Sexuality Information
and Education Council.